706
Views & Citations10
Likes & Shares
Aim: Urinary tract infection (UTI) is a term
applied to a variety of clinical conditions ranging from asymptomatic presence
of bacteria in urine to severe infection of kidney with resultant sepsis.
Despite the widespread availability of antibiotics it remains the most common
bacterial infection in human beings. The aim of this study was to analyze the
bacteriological spectrum of UTI and its antibiogram among patients admitted at
Rawalpindi Institute of Cardiology (RIC).
Material and methods: Urine specimens were taken from
patients of all age groups admitted in Rawalpindi Institute of Cardiology from
January to December 2018. A total of 727 urine specimens were cultured on
Cysteine Lactose Electrolyte Deficient Agar. The growth was identified and
antibiotic susceptibility was carried out by disc diffusion method as per
recommended CLSI guidelines.
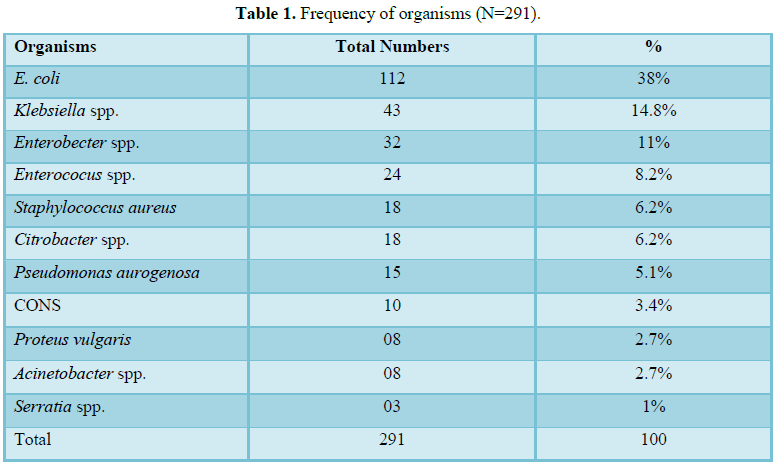
Results: Out of 727 urine specimens, 291 were culture
positive. Escherichia coli was the
most frequent uropathogen (38%) followed by Klebsiella
pneumonia (14.8%), Enterobacter
spp. (11%) and Enterococcus spp.
(8.2%).
Discussion: Urinary tract infection is common among
hospitalized patients. Frequent use of antibiotics has led to antibiotic
resistance against common infections including UTI. However, very little information
is available about UTIs in patients with ischemic heart disease and other
cardiac ailments. Our study has also confirmed UTI being frequent among
hospitalized cardiac patients. Nitrofurantoin was the most effective antibiotic
followed by Imipenem, Meropenem and Amikacin against Enterobacteriacae. Most
isolates showed resistance to Ciprofloxacin and Ampicillin.
Keywords: Urinary tract infection, Escherichia coli, Antibiotics
INTRODUCTION
UTI is associated
with significant mortality and morbidity. About 150 million people develop
urinary tract infection every year [1]. UTI is more common in women than in men
due to the short length of urethra [2].
MATERIALS AND METHODS
All specimens were inoculated on Cysteine
Lactose Electrolyte Deficient (CLED) Agar and incubated at 37°C for 24 h.
Twenty or more colonies on CLED Agar were taken as significant. Antibiotic
susceptibility was carried out by disc diffusion method against Ampicillin,
Amoxicillin/Clavulanate, Trimethoprim/Sulphamethaxazole, Fosfomycin, Amikacin,
Gentamicin, Aztreonam, Nitrofurantoin, Ciprofloxacin, Ceftriaxone, Cefotaxime,
Pipracillin/Tazobactam, Imipenem, Meropenem as recommended in CLSI-M 100 S 26th
edition [6].
RESULTS
Out of 727 urine samples, 327 (45%) were
obtained from females and 400 (55%) from males patients. Among all urine
samples 291 (40%) were culture positive whereas 436 (60%) were culture
negative. Among all positive cultures 150 (51.5%) were from male patients
whereas 141 cases (48.5%) were from females patients.
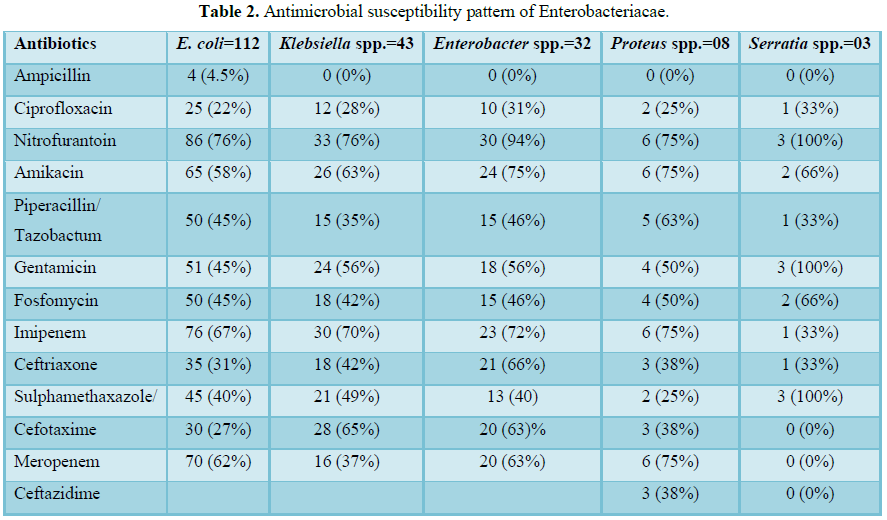
The frequency of various organisms isolated in urine specimens is shown in Table 1. Escherichia coli were the most frequent urinary pathogen followed by Klebsiella spp. and others. E. coli was susceptible to Nitrofurantoin (76%) followed by Imipenem (67%) and Meropenem (62%). It was least susceptible to Ampicillin (4.5%), Ciprofloxacin (22%) and Cefotaxime (30%). Ciprofloxacin was seen least effective against all Enterobacteriacae whereas Nitrofurantoin, Imipenem and Meropenem were found the most effective as per their susceptibility (Table 2).
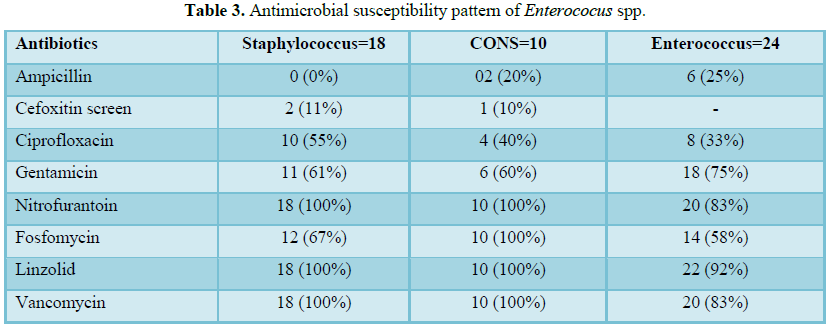
Cefoxitin screen was used to detect Methicillin resistant Staphylococcus aureus (MRSA). All
Staphylococcal isolates were susceptible to Linezolid, Vancomycin and
Nitrofurantoin. Enterococci were least susceptible to Ampicillin and most of
isolates had high level resistance to Gentamycin (Table 3).
Cefoxitin screen was used to detect Methicillin resistant Staphylococcus aureus (MRSA). All
Staphylococcal isolates were susceptible to Linezolid, Vancomycin and
Nitrofurantoin. Enterococci were least susceptible to Ampicillin and most of
isolates had high level resistance to Gentamycin (Table 3).
DISCUSSION
Effective
management of UTI depends upon the identification of microorganism and its
susceptibility. It often requires close cooperation between clinician and
microbiologist [7].
UTI is the most
common bacterial infection and second common cause of morbidity and mortality
in all age groups. In a study from Pakistan Institute of Medical Science, out
of 1363 urine samples 289 were found positive for UTI [8]. Similar findings
were observed in a study from Agha Khan University Hospital, Pakistan, where
out of 9892 urine samples 37% were culture positive [9]. In that study, the
frequency of UTI in females and males was 60.5% and 39.5%, respectively.
However, in our study the gender distribution is 51.5% in males and 48.5% in
females out of total 291 culture positive cases. The frequency of uropathogens
isolated in our study is different from other studies where UTI was more
frequent in females than in males. The clinical factors including anatomic
differences, hormonal effects and behavioral patterns contribute to frequent
UTI [10,11]. Hasan et al. [12] have reported a prevalence rate of UTI in
females (70.5%) and males (29.5%). However, in our study being carried out in a
cardiac hospital, UTI is more frequent in males than in females since
myocardial ischemia is more common in male population than females.
Escherichia coli is the predominant urinary pathogen (38%)
followed by Klebsiella pneumonia (K. pneumonia) (14.8%) in our study. Our
results are similar to that were reported by Patel et al. [13] in Jamnagar,
Gujrat and of Savitha et al. [14], India who had also found E. coli and K. pneumoniae as the most common uropathogen. They found E. coli causing UTI in 53.38% and 48.04%
and Klebsiella spp. in 18.98% and
8.82% of the isolates respectively [15]. Yadav et al. [16] have reported E. coli (61%), followed by S. aureus (12%), CONS (7%), Enterococcus
(5%), K. pneumoniae (5%), Candida spp. (3%), Proteus spp. (2%) and others (6%). The most effective antibiotics
in our study are Nitrofurantoin, Imipenem, Meropenem and Amikacin against
Enterobacteriaceae. Similar findings have been reported by Niranjan et al. in
Puducherry, India [15]. However, Yadav et al. [16] have found Imipenem as the
most effective antibiotic against E. coli
85.9% and against Klebsiella spp.
89.4%.
In a study from
Ethiopia out of 1404 urine samples, 319 (22.7%) were culture positive. Escherichia coli (63.6%) were the
predominant uropathogen. Resistance to Erythromycin, Amoxicillin and
Tetracycline was quite high in that study [17].
Nitrofurantoin is
found as the most effective to treat UTI in our study. Similar findings were
observed in surveillance studies by Sasirekha [18] and Khameneh and Afshar [19]
other Indian studies.
Most of the
organisms showed resistance to Ampicillin and Ciprofloxacin in our study. It
could be attributed to empirical use of these antibiotics to treat common
infections including pneumonias in ischemic patients beside preoperative and
postoperative prophylactic use of these antibiotics in our hospital. Similar
findings have been observed by Nozarian and Abdollahi [20] and Keah et al.
[21]. Resistance to Ampicilin (50.1%) and Cotrimoxazole (22.1%) was observed in
patients with complicated UTI and acute pyelonephritis in a study from United
States [22].
In our study E. coli is susceptible to Nitrofurantoin
(76%) followed by Imipenem (67%) and Meropenem (62%). It is least susceptible
to Ampicillin (4.5%), Ciprofloxacin (22%) and Cefotaxime (30%). Ciprofloxacin
is seen the least effective against all Enterobacteriacae whereas
Nitrofurantoin, Imipenem and Meropenem are found the most effective as per
their susceptibility (Table 2).
Klebsiella spp. is the second most frequently isolated
uropathogen (14.8%). It is most susceptible to Nitrofurantoin (76%), Imipenem
(70%) and Meropenem (65%). Amikacin is more effective than Gentamycin being 63%
% and 56%, respectively. Similar findings have been reported by Patel et al.
[13] and Agha Khan University Hospital [9].
We have found Enterobacter spp. 11% in our culture
isolates whereas it was reported 5% from Agha Khan University hospital, Karachi
Pakistan and 8% by Farooq et al. [9] Nozarian and Abdollahi et al. [20]. The
later had reported sensitivity of Enterobacter
spp. 82.3% and 86.7% to Nitrofurantoin and Amikacin, respectively, whereas it
is 94% and 75%, respectively in our study. Susceptibility towards Imipenem is
72% and Meropenem is 63%. The least susceptibility is observed against
Ampicillin, Ciprofloxacin and Cephalosporins in that order. All isolates of Serratia spp. are susceptible to
Gentamycin, Trimethoprim/Sulphamethoxazole and Nitrofurantoin (100%).
The frequency of S. aureus and CONS in our study is 6.2%
and 3.4%, respectively (Table 2), whereas Yadav et al. [16] have
reported these as 12% and 7%, respectively. MRSA and Methicillin-resistant
Coagulase Negative Staphylococcus (MR CONS) are 11% and 10%, respectively in
our study. While, Yadav et al. [16] have reported these as 33% and 96%,
respectively. All of our Staphylococcal isolates are susceptible to Linezolid,
Vancomycin and Nitrofurantoin whereas Yadav et al. [16] have reported these as
95.2%, 100% and 87.4%, respectively [16].
Enterococcus was
found in 8% of the isolates whereas Yadav et al. [16] have reported it as 6% in
their study. We have found it 93% susceptible against Linezolid and 83% against
Vancomycin and Nitrofurantoin each.
CONCLUSION
UTI is the most common
disease among hospitalized patients around the world. Our study has also confirmed
that UTI is also common in patients admitted in a cardiac hospital. UTI is more
frequent in males than in female patients admitted in our cardiac hospital.
Escherichia coli were the most frequent uropathogen. Most of the isolates were
susceptible to Nitrofurantoin, Imipenem, Meropenem and Amikacin but resistant
to Amoxicillin, Ciprofloxacin and Ceftriaxone.
1. Flores-Mireles
AL, Walker JN, Caparon M, Hultgren SJ (2015) Urinary tract infections:
Epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol
13: 269-284.
2. Al-Achi
A (2008) An introduction to botanical medicines: History, science, uses and
dangers. Westport, Conn.: Praeger Publishers, p: 126.
3. https://www.niddk.nih.gov/health-information/urologic-diseases/kidney-infection-pyelonephritis
4. https://www.niddk.nih.gov/health-information/urologic-diseases/bladder-infection-uti-in-adults
5. Woodford
HJ, George J (2011) Diagnosis and management of urinary infections in older people
(PDF). Clin Med 11: 80-83.
6. Richard
T, Patel JB (2013) Performance standards for antimicrobial. 26th Edn.
7. Water G,
Harrison B, Kunin G (1996) Urinary tract infection. N Engl Med J, pp: 248-250.
8. Amber M,
Shoaib M, Rehman A, Zafar MM, Ain QT, et al. (2016) Comparative study of
causative agents of UTI among indoor, outdoor, children and adult patients of
Pakistani population. Bull Env Pharmacol Life Sci 58: 34-41.
9. Farooqui
B, Alam M, Khurshid M (1989) Urinary tract infection. J Pak Med Assoc 39:
129-131.
10. Miller
O, Hemphill RR (2001) Urinary tract infection and pyelonephritis. Emerg Med
Clin North Am 19: 655-674.
11. Foxman B
(2002) Epidemiology of urinary tract infections: Incidence, morbidity and
economic costs. Am J Med 113: 5-13.
12. Hasan
AS, Nair D, Kaur J, Baweja G, Deb M, et al. (2007) Resistance patterns of
urinary isolates in a tertiary Indian hospital. J Ayub Med Coll Abbottabad 19:
39-41.
13. Patel S,
Taviad PP, Sinha M, Javadekar TB, Chaudhari VP (2012) Urinary tract infections
(UTI) among patients at GG Hospital and Medical College, Jamnagar. Nat J Comm
Med 3: 138-141.
14. Savitha
T, Murugan K, Thangamariappan K (2011) Prevalence study on emergence of urinary
tract infection in Erode, Tamil Nadu, India. Int J Curr Res 2: 5-13.
15. Niranjan
V, Malini A (2014) Antimicrobial resistance pattern in Escherichia coli causing
urinary tract infection among inpatients. Indian J Med Res 139: 945.
16. Yadav M,
Pal R, Damrolien S, Khumanthem SD (2017) Microbial spectrum of urinary tract
infections and its antibiogram in a tertiary care hospital. Int J Res Med Sci
5: 2718-2722.
17. Kibret
M, Abera B (2014) Prevalence and antibiogram of bacterial isolates from urinary
tract infections at Dessie Health Research Laboratory, Ethopia. Asian Pac J
Trop Biomed 4: 164-168.
18. Sasirekha
B (2013) Prevalence of ESBL, AmpC β-lactamases and MRSA among uropathogens and
its antibiogram. EXCLI J 12: 81-88.
19. Khameneh
ZR, Afshar AT (2009) Antimicrobial susceptibility pattern of urinary tract
pathogens. Saudi J Kidney Dis Transplant 20: 251.
20. Nozarian
Z, Abdollahi A (2015) Microbial etiology and antimicrobial susceptibility of bacteria
implicated in urinary tract infection in Tehran, Iran. Iran J Pathol 10: 54.
21. Keah SH,
Wee EC, Chng KS, Keah KC (2007) Antimicrobial susceptibility of
community-acquired uropathogens in general practice. Malays Fam Phisician 2:
64-69.
22. Peterson
J, Kaul S, Khashab M, Fisher A, Kahn JB (2007) Identification and pre-therapy
susceptibility of pathogens in patients with complicated urinary tract
infection or acute pyelonephritis enrolled in a clinical study in the United
States from November 2004 through April 2006. Clin Ther 29: 2215-2221.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- International Journal of Surgery and Invasive Procedures (ISSN:2640-0820)
- Journal of Clinical Trials and Research (ISSN:2637-7373)
- Oncology Clinics and Research (ISSN: 2643-055X)
- Journal of Spine Diseases
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- International Journal of Clinical Case Studies and Reports (ISSN:2641-5771)


